What does chart mean in EMS
 Natalie Ross
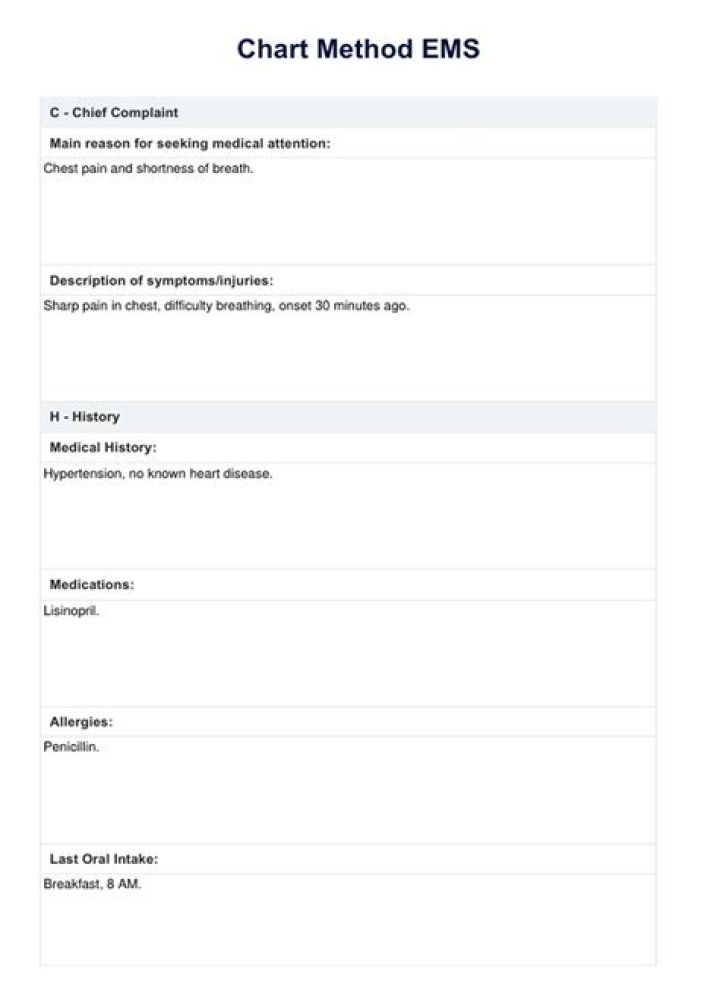
Natalie Ross C.H.A.R.T. C = Chief Complaint. H = History (Past & Present) A = Assessment. R = Rx or Treatment.
What is charting in EMS?
An effective EMS chart informs subsequent caregivers of the patient’s presenting signs and symptoms, the caregiver’s assessment of the patient’s condition, attempted EMS interventions, successful EMS interventions and the patient’s response to those interventions.
How do I write a good EMS report?
- Dispatch & Response Summary. …
- Scene Summary. …
- HPI/Physical Exam. …
- Interventions. …
- Status Change. …
- Safety Summary. …
- Disposition.
What does the R in chart stand for?
An X-bar and R (range) chart is a pair of control charts used with processes that have a subgroup size of two or more. … The X-bar chart shows how the mean or average changes over time and the R chart shows how the range of the subgroups changes over time.What is EMS documentation?
The primary purpose of EMS documentation is to provide a written record of patient assessment and treatment that can help guide further care. For the information to be readily understood and communicated, it must be organized in a format that all healthcare providers involved in patient care will understand.
What is a chart narrative?
Narrative charting is a means of recording patient data that enables doctors and nurses to consult a patient’s status and plan future treatment quickly and effectively. … Each letter in the acronym DAIR represents a step in the information-gathering and treatment procedures: Data, Assessment, Intervention and Response.
What is the chart method?
The charting method is a note-taking method that uses charts to condense and organize notes. It involves splitting a document into several columns and rows which are then filled with summaries of information. This results in a note format that enables efficient comparisons between different topics and ideas.
What does SOAP stand for?
Introduction. The Subjective, Objective, Assessment and Plan (SOAP) note is an acronym representing a widely used method of documentation for healthcare providers.What does the T in CHART stand for?
Definition. CHART. Coordinated Highways Action Response Team.
What is a PCR in EMS?A PCR documents care provided to a patient before they arrive at the hospital. … The primary purpose of the Patient Care Report (PCR) is to document all care and pertinent patient information as well as serving as a data collection tool.
Article first time published onHow do you report a patient?
- Describe the case in a narrative form.
- Provide patient demographics (age, sex, height, weight, race, occupation).
- Avoid patient identifiers (date of birth, initials).
- Describe the patient’s complaint.
- List the patient’s present illness.
- List the patient’s medical history.
When completing your PCR after a call you should?
When completing your PCR after a call, you should: defer the narrative only if the information in the drop-down boxes accurately reflects the assessment and treatment that you performed. complete a thorough and accurate narrative because drop-down boxes cannot provide all of the information that needs to be documented.
Do paramedics make reports?
A verbal report is typically provided by paramedics and documented by triage nurses. Paramedics subsequently complete a patient care report which is submitted electronically.
What does defensive documentation mean?
us. a document explaining why a company’s management thinks that shareholders should not agree to an offer made by another company to take control: Next week’s defence document will detail the bank’s strategy.
How do I file an EMT?
- What was provided.
- When it was provided.
- Patient’s reaction to it.
What is charting in nursing?
Charting in nursing provides a documented medical record of services provided during a patient’s care, including procedures performed, medications administered, diagnostic test results and interactions between the patient and healthcare professionals.
What are the 6 C of charting?
The Six C’s of Medical Records Client’s Words, Clarity, Completeness, Conciseness, Chronological Order and Confidentiality. Client’s Words – a medical assistant should always record the patient’s exact words.
How do you write PCR EMT?
- Be specific. …
- 6 questions EMS leaders must answer about buying an ePCR system.
- 5 costly EMS documentation mistakes.
- Paint a picture of the call. …
- Do not fall into checkbox laziness. …
- Complete the PCR as soon as possible after a call. …
- Proofread, proofread, proofread.
What is focused charting?
Focus Charting – is a method for organizing health information in the individual’s record. It is a systematic approach to documentation, using nursing terminology to describe individual’s health status and nursing action.
What is traditional charting?
Narrative Charting – This is the traditional form of charting. It is a source-oriented record wherein each medical personnel makes documentation on the patient’s record in a separate section. The advantage of using this type of recording is the provision of an organized sections for each member of the healthcare team.
What is charting by exception examples?
For example, a physician claimed she did not record a patient’s temperature because she “charted by exception” and the temperature “must have been normal because she did not write anything”. The clinical evidence, in this case, made her claim suspect.
What is Opqrst in EMT?
Each letter stands for an important line of questioning for the patient assessment. The parts of the mnemonic are: Onset , Provocation/palliation, Quality, Region/Radiation, Severity, and Time.
How do you write a medical chart?
- Keep it legible and professional.
- Beware of EMR laziness.
- It’s all about cause and effect.
- Stop procrastinating.
- Get consent and document it.
- Be complete and specific.
- Document refusal of care and noncompliance.
- Include follow-up instructions.
What is the soap system of charting?
Today, the SOAP note – an acronym for Subjective, Objective, Assessment, and Plan – is the most common method of documentation used by providers to input notes into patients’ medical records. They allow providers to record and share information in a universal, systematic and easy-to-read format.
What is foaming capacity of soaps?
Theory: The foaming capacity of a soap sample depends upon the nature of soap and its concentration. This can be compared for various samples of soaps by taking the same concentration of solution and shaking them. … The lesser the time taken by a solution for the disappearance of foam, the lower is its foaming capacity.
What is another name for SOAP?
- detergent.
- soapsuds.
- castile.
- lather.
- soft soap.
- suds.
What SOAP means Mcq?
SOAP stands for Simple object access protocol and it describes the distributed processing model. There are different nodes used and they are termed as SOAP nodes.
What does a PCR test tell you?
What is a PCR test? PCR means polymerase chain reaction. It’s a test to detect genetic material from a specific organism, such as a virus. The test detects the presence of a virus if you have the virus at the time of the test.
What is minimum data set EMS?
Patient care reports should include what is known as a minimum data set, or the absolute least amount of information possible, to facilitate correct tracking of EMS data by the National EMS Information System.
Why do we do PCR?
PCR is very important for the identification of criminals and the collection of organic crime scene evidence such as blood, hair, pollen, semen and soil. … PCR allows DNA to be identified from tiny samples – a single molecule of DNA can be enough for PCR amplification.
What medical report means?
Noun. 1. medical report – a report of the results of a medical examination of a patient. report, written report, study – a written document describing the findings of some individual or group; “this accords with the recent study by Hill and Dale” Based on WordNet 3.0, Farlex clipart collection.